Poets CF, Hogeveen M, Schwindt S, Mader S, Härtel C, van den Hoogen A
Click on the image to read the standard in brief.
Target group
Infants requiring intensive care and parents
User group
Healthcare professionals, neonatal units, hospitals, and health services
Statement of standard
Nurse staffing levels reflect the needs of the infants they are caring for, which include one to one nursing during intensive care and one to two nursing during intermediate care.
Rationale
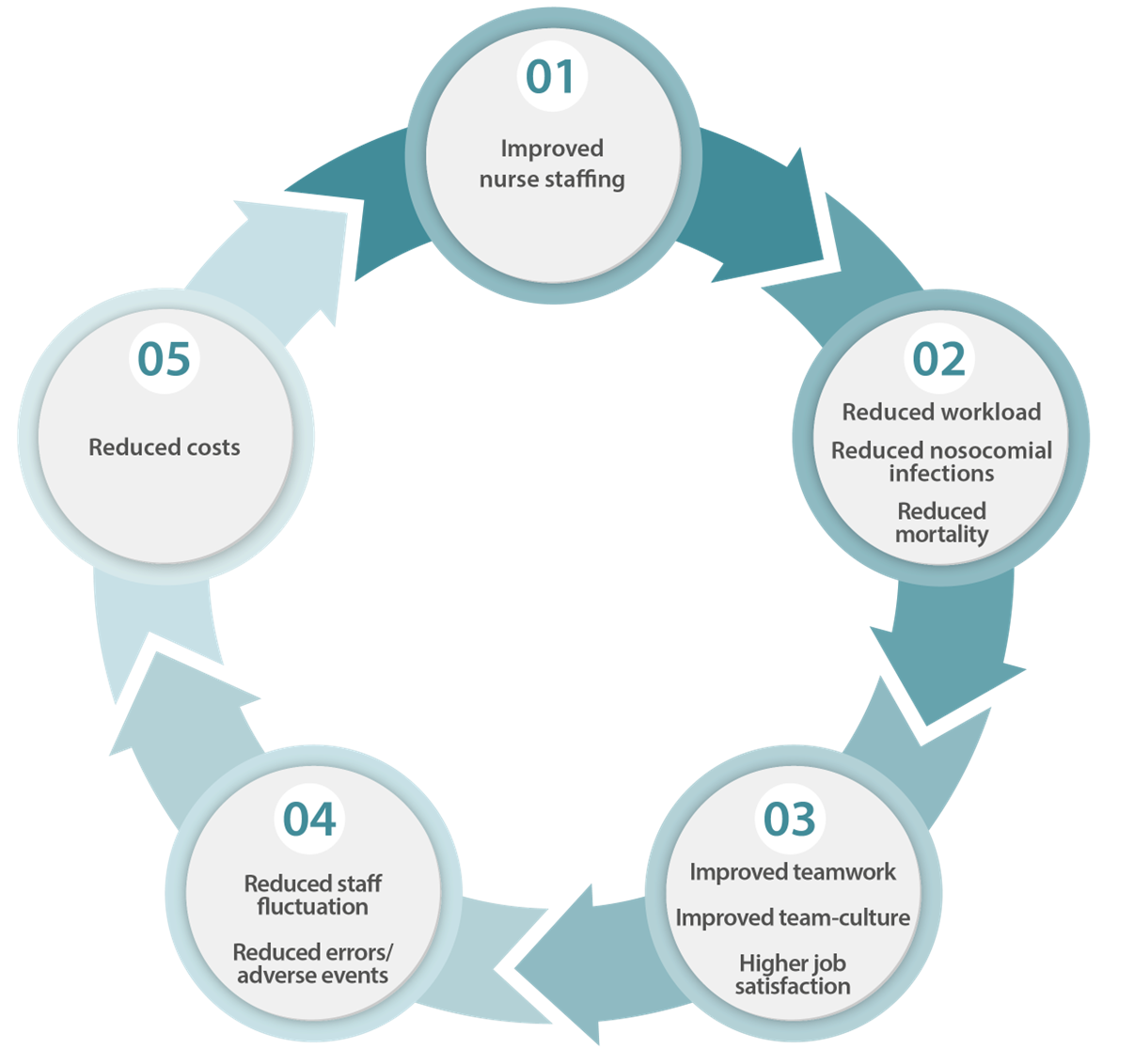
At present, nurse staffing levels vary widely between neonatal services. (1,2) The definition of levels varies also between countries. A useful example for defining the different levels of neonatal care has been provided by the British Association of Perinatal Care. (3) There is evidence that insufficient nursing numbers are associated with increased mortality and increased infection rates. (4–10) Data indicate that provision of sufficient nursing staff will facilitate the timely delivery of neonatal care(4), allow for better prevention of nosocomial infections(11–13), results in better compliance with set oxygen saturation targets(6) and improved hand hygiene compliance. (14) There is also a relationship between the proportion of one to one nursing achieved and mortality. (15) Finally, and also important in this context, job satisfaction was found to be higher if nurses perceive their staffing level as adequate, which in turn can lead to higher levels of patient safety and thus, cost reductions (see Figure 1). (16–18)
Figure 1: Effects of improved nursing staff provision
Evidence-based standards in this area include:
an agreed proportion of nurses working in the NICU should have 3-5 years work experience in a NICU or completed post-registration education in intensive care(3,19)
a nurse-to-infant ratio of one to one(16,19) (one nurse for one infant) for infants requiring intensive care, of one to two(16,19) (one nurse for two infants) for infants needing intermediate care, and a ratio of at least one to four for all infants requiring special care (16)
in addition to nursing staff, support should be available from professionals with specific expertise in neonatal practice in the following areas: social work, psychology, dietetics, physiotherapy, speech and language therapy, pharmacy, as well as nursing aids and lactation consultants (see Infant-and family-centred developmental care) (16,19–23)
Benefits
Short-term benefits
Timely delivery of neonatal care (4)
Reduced risk of nosocomial infections(11–13)
Improved compliance with set oxygen saturation targets in infants (6)
Improved hand hygiene compliance (14)
Reduced neonatal mortality(9)
Long-term benefits
Improved long-term outcomes (7)
Improved job satisfaction of nursing staff (16)
Components of the standard
Component
Grading of evidence
Indicator of meeting the standard
For parents and family
Parents are supported to be the primary caregiver. (24)
A (Low-Moderate quality) B (Moderate quality)
Parent feedback
For healthcare professionals
Patient’s care has priority over administrative and housekeeping tasks for nurses in clinical care.
B (High quality)
Guideline
For neonatal unit
A unit guideline on nurse staffing requirements is available and regularly updated.
B (High quality)
Guideline
Sufficient nurse staffing numbers to provide appropriate levels of neonatal care is ensured:(16,19)
One nurse to one patient for intensive care (15)
One nurse to two patients for intermediate care
One nurse to four patients during special care
In addition, one nurse to provide shift coordination
A (High quality) C (Moderate quality)
Audit report1
For hospital
Sufficient nurse staffing numbers for care and continuing professional development and education of staff is ensured (see Education & training). (16,19)
A (Moderate quality)
Audit report1, training documentation
For health service
A national guideline on nurse staffing requirements is available and regularly updated.
B (High quality)
Guideline
The staffing required by a unit is defined according to the number of beds and the care level of the beds. (16,19)
A (Moderate quality) C (Moderate quality)
Audit report1
Adequate national or regional training places on accredited educational courses are ensured (see Education & training).
A (Moderate quality) B (High quality)
Audit report1
1The indicator “audit report” can also be defined as a benchmarking report.
Where to go
Further development
Grading of evidence
For parents and family
N/A
For healthcare professionals
N/A
For neonatal unit
N/A
For hospital and health service
Develop initiatives to make neonatal nursing attractive as a career option.
B (High quality)
Develop evidence-based standards for medical and allied professional staffing. (25)
A (High quality))
Agree and implement a national or regional policy to ensure appropriate nurse staffing numbers. (16)
A (High quality)
Getting started
Initial steps
For parents and family
National parent representatives contribute to national consensus meetings on neonatal staffing.
Involve parents in basic care procedures from very early on during neonatal care provision. (24)
For healthcare professionals
N/A
For neonatal unit
Develop and implement a unit guideline on nurse staffing requirements.
Inform health services and stakeholders about the importance of appropriate NICU staff numbers.
For hospital
Develop and educate nursing workforce.
Facilitate development of neonatal expertise by allied professionals.
For health service
Develop and implement a national guideline on nurse staffing requirements.
Organise expert stakeholder groups on a national level to reach consensus about nursing, medical and allied professional neonatal staffing requirements and their implementation.
Patry C, Schindler M, Reinhard J, Hien S, Demirakca S, Böhler T, et al. A gap between Need and Reality: Neonatal Nursing Staff Requirements on a German Intensive Care Unit. Pediatr Rep. 2014 Feb 17;6(1):5186.
Corchia C, Fanelli S, Gagliardi L, Bellù R, Zangrandi A, Persico A, et al. Work environment, volume of activity and staffing in neonatal intensive care units in Italy: results of the SONAR-nurse study. Ital J Pediatr. 2016 Apr 2;42:34.
British Association of Perinatal Medicine. Service standards for the organisation of perionatal care, 3rd ed. London 2010.
Pillay T, Nightingale P, Owen S, Kirby D, Spencer A. Neonatal nurse staffing and delivery of clinical care in the SSBC Newborn Network. Arch Dis Child Fetal Neonatal Ed. 2012 May;97(3):F174-178.
Cimiotti JP, Haas J, Saiman L, Larson EL. Impact of staffing on bloodstream infections in the neonatal intensive care unit. Arch Pediatr Adolesc Med. 2006 Aug;160(8):832–6.
Sink DW, Hope SAE, Hagadorn JI. Nurse:patient ratio and achievement of oxygen saturation goals in premature infants. Arch Dis Child Fetal Neonatal Ed. 2011 Mar;96(2):F93-98.
Beltempo M, Lacroix G, Cabot M, Blais R, Piedboeuf B. Association of nursing overtime, nurse staffing and unit occupancy with medical incidents and outcomes of very preterm infants. J Perinatol Off J Calif Perinat Assoc. 2018 Feb;38(2):175–80.
Leistner R, Thürnagel S, Schwab F, Piening B, Gastmeier P, Geffers C. The impact of staffing on central venous catheter-associated bloodstream infections in preterm neonates – results of nation-wide cohort study in Germany. Antimicrob Resist Infect Control. 2013 Apr 4;2(1):11.
Hamilton KESC, Redshaw ME, Tarnow-Mordi W. Nurse staffing in relation to risk-adjusted mortality in neonatal care. Arch Dis Child Fetal Neonatal Ed. 2007 Mar;92(2):F99–103.
Sherenian M, Profit J, Schmidt B, Suh S, Xiao R, Zupancic JAF, et al. Nurse-to-patient ratios and neonatal outcomes: a brief systematic review. Neonatology. 2013;104(3):179–83.
Rogowski JA, Staiger D, Patrick T, Horbar J, Kenny M, Lake ET. Nurse staffing and NICU infection rates. JAMA Pediatr. 2013 May;167(5):444–50.
Lake ET, Staiger D, Horbar J, Kenny MJ, Patrick T, Rogowski JA. Disparities in perinatal quality outcomes for very low birth weight infants in neonatal intensive care. Health Serv Res. 2015 Apr;50(2):374–97.
The UK Neonatal Staffing Study Group. Relationship between probable nosocomial bacteraemia and organisational and structural factors in UK neonatal intensive care units. Qual Saf Health Care. 2005 Aug 1;14(4):264–9.
Pessoa-Silva CL, Toscano CM, Moreira BM, Santos AL, Frota ACC, Solari CA, et al. Infection due to extended-spectrum beta-lactamase-producing Salmonella enterica subsp. enterica serotype infantis in a neonatal unit. J Pediatr. 2002 Sep;141(3):381–7.
Watson SI, Arulampalam W, Petrou S, Marlow N, Morgan AS, Draper ES, et al. The effects of a one-to-one nurse-to-patient ratio on the mortality rate in neonatal intensive care: a retrospective, longitudinal, population-based study. Arch Dis Child Fetal Neonatal Ed. 2016 May;101(3):F195-200.
Kalisch BJ, Lee H, Rochman M. Nursing staff teamwork and job satisfaction. J Nurs Managem 2010;18:938-47
Berry JC, Davis JT, Bartman T, Hafer CC, Lieb LM, Khan N et al. Improved Safety Culture and Teamwork Climate Are Associated With Decreases in Patient Harm and Hospital Mortality Across a Hospital System. J Patient Saf. 2020 Jun;16(2):130-136.
De Bienassis K, Slawomirski L, Klazinga NS. Organisation for Economic Co-operation and Development. The economics of patient safety Part IV: Safety in the workplace: Occupational safety as the bedrock of resilient health systems. OECD Health Working Papers. 2021. Report No.: No. 130.
Please enter your job description and origin country
You are currently viewing a placeholder content from Facebook. To access the actual content, click the button below. Please note that doing so will share data with third-party providers.
You are currently viewing a placeholder content from Instagram. To access the actual content, click the button below. Please note that doing so will share data with third-party providers.
You are currently viewing a placeholder content from X. To access the actual content, click the button below. Please note that doing so will share data with third-party providers.