< Back to Patient safety & hygiene practice
Authors
Mileder L, Schwindt E, Hogeveen M, Thiele N, Ares S

Neonates, infants, parents, and families
Healthcare professionals, neonatal units, hospitals, and health services
Patient safety and quality improvement activities need to be fully integrated in clinical practice.
Infants admitted to a neonatal intensive care unit (NICU) are at a high risk of being harmed by lapses in quality or safety. (1) Specific issues of neonatal patient safety include medication and nutrition errors, errors in respiratory care, infections due to invasive procedures and neonatal care in general, patient identification errors, and diagnostic errors. (2)
Improving patient safety is an important component of high-quality care and requires a safety-oriented culture and the support of an appropriate system for the identification of, investigation of, and learning from quality issues. (3) Although there are several schemes for quality improvement, awareness, local leadership and implementation are critical to improving outcomes for ill neonates and infants. (4-9) Furthermore, structure, data monitoring, and culture are important determinants of any quality programme in neonatal care. (10)
A quality system needs to be championed at the hospital board level but is led from within the interprofessional neonatal team, supported by the quality improvement staff. Structural components include dedicated education and training as well as a system capturing data to monitor key indicators as prioritised by the neonatal team. The healthcare team should develop a safety culture in which transparency, blame-free reporting and the development of learning from clinical events reported within the system are valued. Units and hospitals should establish an advisory board to coordinate and direct quality improvement initiatives.
For parents and family
B (Moderate quality)
Patient information sheet1
B (Moderate quality)
Parent feedback
B (Moderate quality)
Training documentation
B (Moderate quality)
Parent feedback
B (Moderate quality)
Guideline
For healthcare professionals
B (Moderate quality)
Guideline
B (Moderate quality)
Training documentation
B (Moderate quality)
Audit report2, guideline, training documentation
B (Moderate quality)
Audit report2, clinical records
B (Moderate quality)
Staff feedback
B (Moderate quality)
Guideline
B (Moderate quality)
Healthcare professional feedback, minutes of debriefing
For neonatal unit
B (Moderate quality)
Guideline
B (Moderate quality)
Audit report2, guideline
B (Moderate quality)
Audit report2, guideline
B (Moderate quality)
Audit report2, guideline
B (Moderate quality)
Audit report2, training documentation
B (Moderate quality)
Audit report2, clinical records
For hospital
B (Moderate quality)
Training documentation
B (Moderate quality)
Guideline, audit report2
B (Moderate quality)
Guideline, audit report2
B (Moderate quality)
Audit report2
B (Moderate quality)
Audit report2
For health service
B (Moderate quality)
Guideline
B (Moderate quality)
Audit reports2
1The indicator “patient information sheet” is an example for written, detailed information, in which digital solutions are included, such as web-based systems, apps, brochures, information leaflets, and booklets.
2The indicator “audit report” can also be defined as a benchmarking report.
For parents and family
A (Moderate quality)
For healthcare professionals
A (Low quality)
A (Low quality)
A (Low quality)
For neonatal unit
A (Moderate quality)
For hospital
A (Moderate quality)
For health service
B (Moderate quality)
For parents and family
For healthcare professionals
For neonatal unit
For hospital
For health service
A lot of attention is being dedicated to improving the quality of neonatal care, as the extremely vulnerable and seriously ill patients in a NICU are at a high risk of being harmed by lapses in quality or safety. Nevertheless, improving healthcare quality has proven to be a challenging undertaking that foremost requires long-term dedication. It has become clear that the science of improvement, human factors, and implementation are indispensable in increasing the quality of care and patient safety. While acknowledging that no single system will fit all NICUs, this standard attempts to highlight the most relevant topics and tools that NICUs can apply in their quest for quality management and improvement.
Since the publication of the landmark report “To err is human”(4), the quality and patient safety movement, which had taken off with a slow start, has gained more and more momentum. Numerous initiatives and organisations dedicated to quality improvement have been created, such as the Institute for Healthcare Improvement in the USA and the Health Foundation in the UK. Research in the fields of healthcare quality, patient safety, implementation, innovation, and human factors has exploded. As the research and knowledge of safety and quality has increasingly been shared, it became evident that a number of basic requirements for improvement are necessary for all healthcare settings.
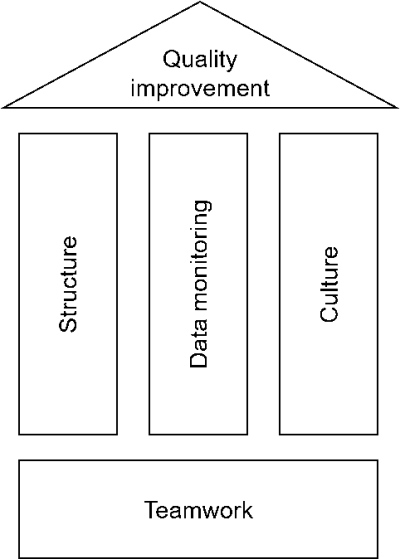
First of all, a system or structure for Quality and Patient Safety Management (QPSM) needs to be in place. Roles, tasks and responsibilities have to be defined. It needs to be clear who is doing what, and who is accountable for which components of the management system. This needs to be facilitated and supported actively by boards, directors, and (middle) management; quality management will undoubtedly fail when it is simply added to the everyday tasks and activities of the engaged frontline staff. Another necessity relates to improving skills. Frontline staff and management involved in quality improvement need to collaborate with co-workers schooled in change management, as healthcare professionals usually are not trained in the skills for developing and implementing new processes, procedures etc.
Next to this, each NICU needs to determine what data to monitor and in what way. In order to be able to prioritise, implement, monitor, adapt and create success of any improvement initiative, quantitative data, which is relevant to the addressed problem, need to be collected objectively (see standard “Quality indicators”).
The last pillar of QPSM is culture. How is the safety climate in a NICU, a hospital, a country? Is there a “just culture” (5,36) where openly discussing errors and mistakes is not only possible without fear for repercussions, but in fact welcomed as an opportunity to learn? In this respect, leading by example is one of the most powerful modes of improving the safety culture in any setting. Directors and heads of departments that welcome feedback on their own deficiencies and lack of adhering to relevant standards and guidelines will likely see an increase in commitment from frontline staff and patients/parents. Next to leadership in setting the standard for the desired work-related behaviours, they also need to facilitate regular teamwork and team-oriented training. Teamwork is more and more recognised as the foundation of healthcare and, thus, needs to be consistently addressed. (17) As has been proven numerous times, expert teamwork is not created by simply putting a number of experts together, but requires training, both in acute care settings such as the NICU as well as in other settings such as for instance an outpatient department. (37) Healthcare frontline staff are well trained professionals in their field of expertise, however, the non-technical skills that are required for effective teamwork quite often have not received the attention they require. Communication, leadership, decision-making, stress and risk management, as well as developing a shared understanding of the situation are topics of training, education, and discussion that must be addressed. Especially interdisciplinary and interprofessional simulation training allows training and rehearsing these essential non-technical skills. (38,39) Debriefing of actual clinical events further supports teamwork improvement. (26-28)
Improving patient safety, teamwork, and unit culture also relate to the notion that patients and families should be welcomed as members of the team, as, for example, medication errors are more often recognized in integrated care. (12) Therefore, engaging parents “as partners in safety” has been suggested to improve the safety of neonatal care. (40) Shared decision making is another integral part of patient and parent engagement. (41) However, integrating parents in the NICU team can be quite challenging and there may be a number of barriers. For instance, the events surrounding the birth of a preterm child can be extremely stressing for parents, thus decreasing their ability to make shared decisions, or the frontline staff feel they cannot properly discuss the decisions during the rounds if the parents are present. These potential issues obviously need to be explored and dealt with before teaming up with parents can reach its full potential. Several initiatives have been launched worldwide, so what remains is learning from each other, and from the parents/families, in how to best achieve safe, patient-centred and reliable care for the most vulnerable, i.e. the NICU patients. (42)
Second edition, December 2024. Previous edition reviewed by Associate Professor Nicole Yamada.
Lifecycle
5 years/next revision: 2029
Recommended citation
GFCNI, Mileder L et al., European Standards of Care for Newborn Health: Patient safety and quality awareness in neonatal intensive care. 2024.
You are currently viewing a placeholder content from Facebook. To access the actual content, click the button below. Please note that doing so will share data with third-party providers.
More InformationYou are currently viewing a placeholder content from Instagram. To access the actual content, click the button below. Please note that doing so will share data with third-party providers.
More InformationYou are currently viewing a placeholder content from X. To access the actual content, click the button below. Please note that doing so will share data with third-party providers.
More Information