Andritsou F, Oude-Reimer M, Camba F, Ceccatelli M, Nagy Bonnard L, Hankes-Drielsma I, Jørgensen E, Silva E
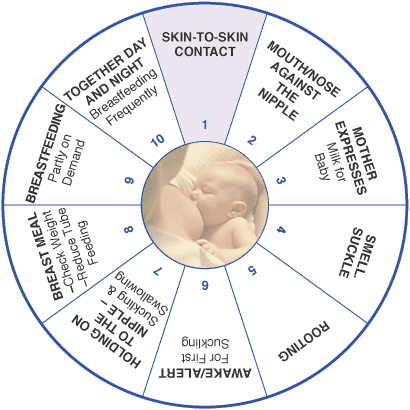
Click on the image to read the standard in brief.
Target group
Infants, parents, and families
User group
Healthcare professionals, neonatal units, hospitals, and health services & stakeholders
Statement of standard
All mothers are supported to feed their infants exclusively with human milk (expressed mother’s milk or donor human milk) during the hospital stay and after discharge.
Rationale
Breastfeeding is the biological norm for all mammals, including humans and it is the natural way of providing nurturing, nutrients, and energy needed for physical and neurological growth and development. Exclusive breastfeeding gives every infant and child the right to the highest standard of health and a fair start in life, without inequalities or social injustice. (1,2)
By receiving evidence-based information and lactation counselling, nursing parents can be enabled to breastfeed and express milk, if they feel supported by their partner, family, the healthcare system and society at large, and are protected from commercial interests that negatively impact on breastfeeding. (3) Staff needs to enable informed decision-making while remaining sensitive to maternal choice and providing alternative solutions like donor human milk for women who are unable to provide any or sufficient breastmilk (see standard Providing mother’s own milk for preterm and ill term infants).
Initiation of breastfeeding within the first hour after birth or as soon as possible and immediate and uninterrupted skin-to-skin contact are important for the establishment of breastfeeding, to facilitate mother and infant bonding, and for newborn infants’ and children’s survival and development. (3,4) The early initiation of breastfeeding results in early and successful expression of colostrum, the ‘very first food’ and the perfect food for every newborn infant, as WHO recommended and stated. (3)
Mothers are supported in their decision how to feed their infants. Regarding that exclusive breastfeeding is recommended from WHO and AAP for at least the first 6 months of life and up to 2 years of age. After the first six months breastfeeding is recommended as long as both, mother and child are comfortable with this. This is often culturally and societally based. (1,5)
The Baby Friendly Hospital Initiative (BFHI) is a global effort that focuses on providing optimal clinical care for new mothers and their infants. The initiative was launched by WHO and UNICEF in 1991, following the Innocent Declaration of 1990. The Baby-friendly initiative helps and motivates maternity and infant services, and facilities worldwide to implement practices that provide optimal breastfeeding care for mothers and infants. (6) All hospitals are eligible to seek BFHI accreditation. (7)
Benefits
Short-term benefits
Improved growth and neurodevelopment (see Nutrition) (7)
Reduced risk of necrotising enterocolitis and late-onset sepsis (8-10)
Improved mother-infant bonding (11)
Reduced neonatal mortality and infections in term infants (12)
Long-term benefits
Reduced risk for overweight or obesity (13)
Reduced risk of mortality due to diarrhoea and other infections (14)
Improved intelligence tests and higher school attendance (15)
Improved child development and reduced health costs (16)
Reduced risk of breast cancer following a period of breastfeeding (17,18)
Improved confidence and mental health for mothers (19)
Components of the standard
Component
Grading of evidence
Indicator of meeting the standard
For parents and family
All pregnant women and their partners are supported antenatally by healthcare professionals to understand the connection between labour interventions and lactation, and to recognise the value and the benefits of breastfeeding and early relationships. (20,21)
A (High quality) B (High quality)
Patient information sheet, training documentation
Parents are informed and guided by healthcare professionals before or directly after birth on early initiation of skin-to-skin care (where possible), positioning and attachment, hand-expression, responsive feeding, potential challenges of breastfeeding a preterm infant, informed decision-making regarding the introduction of donor human milk, artificial formula, nutritional supplements, or fluids other than breastmilk. (6,22)
A (High quality) B (High quality)
Guideline, patient information sheet1, training documentation
For healthcare professionals
A unit guideline on breastfeeding and expression, and non-nutritive sucking until breastfeeding is established and adhered to by all responsible healthcare professionals. (22)
A (High quality) B (High quality)
Guideline
Training on the importance of breastfeeding and how to use listening and learning skills for counselling a nursing parent, building confidence, and giving emotional and practical support is attended by all responsible healthcare professionals. (4)
B (High quality)
Training documentation
All infants (including term and preterm) are supported to be placed in direct skin-to-skin contact with their mothers immediately following birth for at least an hour (where possible), where possible, to encourage oxytocin release by establishing a zero separation policy that promotes the initiation of breastfeeding and bonding. (23–25)
A (High quality) B (High quality)
Guideline
All infants receive no other milk than human milk (mother’s or donor’s) for at least 24 hours after birth, unless other forms of feeding are medically indicated (see Nutrition) (6)
A (High quality) B (High quality)
Clinical records, guideline
Breastfeeding is encouraged on demand without limiting breastfeeding time schedule unless medically indicated (see Nutrition) (26)
A (Moderate quality)
Clinical records, guideline
Feeding bottles, teats, and pacifiers are not offered to infants whose mothers wish to exclusively breastfeed unless the mother has given consent and has been counselled on their benefits and risks. With professional respect and support on parents’ decision in regards to feeding, alternative methods of feeding are also discussed. (12)
A (Moderate quality) B (High quality)
Clinical records, guideline
For neonatal unit
A unit guideline for supporting breastfeeding and milk expression in all infants is available and regularly updated. For preterm infants who are unable to breastfeed directly, oral stimulation and non-nutritive sucking that involve the use of pacifiers, a gloved finger or a breast that is not yet producing milk are encouraged until breastfeeding is established, and for stress and pain reduction for the infant. (22)
A (High quality) B (High quality)
Guideline
Appropriate facilities to support the expression and storage of mother’s milk are available. (see NICU design)
B (High quality)
Audit report2
Implementation of an education programme, sufficient knowledge, competence, and practical skills that cover all breastfeeding standards are provided to all responsible healthcare professionals. (3,27)
B (High quality)
Training documentation
A preterm infant nutrition and lactation core team with Lactation Consultants and healthcare professionals trained in breastfeeding who support breastfeeding for parents and respect informed decision-making is established. (26)
A (High quality) B (High quality)
Clinical records, guideline
For hospital
A written policy that covers all WHO and UNICEF breastfeeding standards is established and communicated to staff and parents. Established facility policies drive consistent practice during and after the hospital stay to achieve equal and appropriate care. (4,27)
A (High quality) B (High quality)
Policy statement, training documentation
The International Code of Marketing of Breastmilk Substitutes and protective mechanisms from the pervasive advertising of breastmilk substitutes, bottles, teats, or pacifiers in any part of the facility or by any of the staff are fully complied. (1,12)
A (High quality)
Audit report2, guideline
Breastfeeding training programmes for healthcare professionals working in clinical and community settings is provided and all relevant services are supported and funded. (27)
A (High quality) B (High quality)
Guideline, training documentation
Continuous monitoring and data-management systems are in place to monitor compliance and quality improvement. (27)
B (High quality)
Audit report2
Appropriate facilities to support the expression of mother’s milk are available, including private rooms/space for breastfeeding and expressing milk (see Nutrition, NICU design).
B (High quality)
Audit report2
Accreditation by the WHO & UNICEF Baby Friendly Hospital Initiative (BFHI) is in place. (28)
B (High quality)
Audit report2, certificates of award
For health service & stakeholders
A national strategy to improve infant and children feeding practices from governments and political parties that through national policies and legislation will commit actions supporting breastfeeding is in place and regularly updated. (12,27)
A (High quality) B (High quality)
Guideline, national policy
Post discharge breastfeeding support and support for breastfeeding alternatives from skilled healthcare professionals based in the community is provided. (29,30)
A (Moderate quality) B (High quality)
Audit report2, guideline
1The indicator “patient information sheet” is an example for written, detailed information, in which digital solutions are included, such as web-based systems, apps, brochures, information leaflets, and booklets.
2The indicator “audit report” can also be defined as a benchmarking report.
Where to go
Further development
Grading of evidence
For parents and family
Continuous collaboration between parents and healthcare professionals with regard to the breastfeeding wheel is established. (22)
A (Low quality) B (Moderate quality)
For healthcare professionals
N/A
For neonatal unit
Peer-to-peer support and parent groups who experienced a NICU stay are provided in NICU and after discharge. (31,32)
A (High quality) B (Low quality)
For hospital
Liaise with special breastfeeding care services in the community with Lactation Consultants for parents after discharge.
B (High quality)
For health service & stakeholders
Develop a policy to support exclusive breastfeeding for at least six months. (33)
A (High quality) B (Moderate quality)
Develop a national policy and legislation that could commit maternity leave policies for at least 6 months and paid parental leave. (27)
A (High quality) B (Moderate quality)
Support research on breastfeeding and commit to undertake an infant feeding survey.
A (High quality) B (Moderate quality)
Sustainably fund universal breastfeeding support programmes and charitable organisations who play a key-role in supporting families and communities that campaign towards infant’s feeding.
A (High quality) B (Moderate quality)
Getting started
Initial steps
For parents and family
Parents are informed verbally and in writing about the importance and benefits of breastfeeding.
Parents are encouraged to initiate skin-to-skin contact immediately after birth, where possible.
Mothers and nursing parents are guided to understand the newborn’s responsivefeeding cues and behaviours.
For healthcare professionals
Attend training on the importance of breastfeeding and how to encourage and guide mothers to breastfeed and express breastmilk.
For neonatal unit
Develop and implement a unit guideline on breastfeeding and breastmilk expression including transition from non-nutritive to nutritive sucking.
Develop information material on the benefits of breastfeeding.
Provide appropriate equipment for expression of mother’s milk.
For hospital
Support healthcare professionals to participate in training on the importance of breastfeeding and how to encourage and guide mothers to breastfeed and express breastmilk.
For health service
Develop and implement a national guideline on breastfeeding and expression.
Develop awareness-campaigns and educational programmes for parents and healthcare professionals regarding the benefits of breastfeeding.
Breastfeeding wheel (23)
Language and gender
To better reflect the current reality, this statement reflects the changes in language that occurred over the last decade. For this edition, the words “mother”, “mother’s milk”, or “breastfeeding” are used together with more inclusive terms such as “nursing parent”. We acknowledge that our work and care include a wide range of parents and nurturing families.
World Health Organization, International W, Fund (UNICEF) UNC. The baby-friendly hospital initiative : monitoring and reassessment : tools to sustain progress [Internet]. World Health Organization; 1999 [cited 2023 Jul 7]. Report No.: WHO/NHD/99.2. Available from: https://apps.who.int/iris/handle/10665/65380
World Health Organization. Standards for improving quality of maternal and newborn care in health facilities [Internet]. Geneva: World Health Organization; 2016 [cited 2023 Jul 7]. 73 p. Available from: https://apps.who.int/iris/handle/10665/249155
World Health Organization. Guideline: protecting, promoting and supporting breastfeeding in facilities providing maternity and newborn services [Internet]. Geneva: World Health Organization; 2017 [cited 2023 Jul 7]. 120 p. Available from: https://apps.who.int/iris/handle/10665/259386
World Health Organization, Fund (UNICEF) UNC. Protecting, promoting and supporting breast-feeding : the special role of maternity services [Internet]. World Health Organization; 1989 [cited 2023 Jul 7]. Available from: https://apps.who.int/iris/handle/10665/39679
Fallon EM, Nehra D, Potemkin AK, Gura KM, Simpser E, Compher C, et al. A.S.P.E.N. clinical guidelines: nutrition support of neonatal patients at risk for necrotizing enterocolitis. JPEN J Parenter Enteral Nutr. 2012 Sep;36(5):506–23.
Oddy WH. Breastfeeding protects against illness and infection in infants and children: a review of the evidence. Breastfeed Rev Prof Publ Nurs Mothers Assoc Aust. 2001 Jul;9(2):11–8.
Cacho NT, Parker LA, Neu J. Necrotizing Enterocolitis and Human Milk Feeding: A Systematic Review. Clin Perinatol. 2017 Mar;44(1):49–67.
Schwarze CE, Hellhammer DH, Stroehle V, Lieb K, Mobascher A. Lack of Breastfeeding: A Potential Risk Factor in the Multifactorial Genesis of Borderline Personality Disorder and Impaired Maternal Bonding. J Personal Disord. 2015 Oct;29(5):610–26.
Uwaezuoke SN, Eneh CI, Ndu IK. Relationship Between Exclusive Breastfeeding and Lower Risk of Childhood Obesity: A Narrative Review of Published Evidence. Clin Med Insights Pediatr. 2017;11:1179556517690196.
Raheem RA, Binns CW, Chih HJ. Protective effects of breastfeeding against acute respiratory tract infections and diarrhoea: Findings of a cohort study. J Paediatr Child Health. 2017 Mar;53(3):271–6.
Horta BL, Loret de Mola C, Victora CG. Breastfeeding and intelligence: a systematic review and meta-analysis. Acta Paediatr Oslo Nor 1992. 2015 Dec;104(467):14–9.
Victora CG, Horta BL, de Mola CL, Quevedo L, Pinheiro RT, Gigante DP, et al. Association between breastfeeding and intelligence, educational attainment, and income at 30 years of age: a prospective birth cohort study from Brazil. Lancet Glob Health. 2015;3(4):e199–e205.
Chowdhury R, Sinha B, Sankar MJ, Taneja S, Bhandari N, Rollins N, et al. Breastfeeding and maternal health outcomes: a systematic review and meta-analysis. Acta Paediatr. 2015 Dec;104:96–113.
Victora CG, Bahl R, Barros AJ, França GV, Horton S, Krasevec J, et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. The Lancet. 2016;387(10017):475–490.
Tucker Z, O’Malley C. Mental Health Benefits of Breastfeeding: A Literature Review. Cureus. 2022 Sep;14(9):e29199.
Lumbiganon P, Martis R, Laopaiboon M, Festin MR, Ho JJ, Hakimi M. Antenatal breastfeeding education for increasing breastfeeding duration. Cochrane Database Syst Rev. 2016 06;12:CD006425.
Becker GE, Smith HA, Cooney F. Methods of milk expression for lactating women. Cochrane Database Syst Rev. 2016 Sep 29;9:CD006170.
Oras P, Thernström Blomqvist Y, Hedberg Nyqvist K, Gradin M, Rubertsson C, Hellström-Westas L, et al. Skin-to-skin contact is associated with earlier breastfeeding attainment in preterm infants. Acta Paediatr Oslo Nor 1992. 2016 Jul;105(7):783–9.
Cong X, Ludington-Hoe SM, Hussain N, Cusson RM, Walsh S, Vazquez V, et al. Parental oxytocin responses during skin-to-skin contact in pre-term infants. Early Hum Dev. 2015 Jul;91(7):401–6.
EFCNI, Kostenzer J, von Rosenstiel-Pulver C, Hoffmann J, Walsh A, Fügenschuh S, et al. Zero separation. Together for better care! Infant and family-centred developmental care in times of COVID-19 – A global survey of parents’ experiences Project Report. EFCNI; 2021.
Meier PP, Johnson TJ, Patel AL, Rossman B. Evidence-Based Methods That Promote Human Milk Feeding of Preterm Infants: An Expert Review. Clin Perinatol. 2017 Mar;44(1):1–22.
World Health Organization. National implementation of the baby-friendly hospital initiative [Internet]. World Health Organization; 2017 [cited 2023 Jul 7]. 60 p. Available from: https://apps.who.int/iris/handle/10665/255197
Fleurant E, Schoeny M, Hoban R, Asiodu IV, Riley B, Meier PP, et al. Barriers to Human Milk Feeding at Discharge of Very-Low-Birth-Weight Infants: Maternal Goal Setting as a Key Social Factor. Breastfeed Med Off J Acad Breastfeed Med. 2017 Feb;12:20–7.
Briere C-E, McGrath JM, Cong X, Brownell E, Cusson R. Direct-breastfeeding in the neonatal intensive care unit and breastfeeding duration for premature infants. Appl Nurs Res ANR. 2016;32:47–51.
Hall SL, Ryan DJ, Beatty J, Grubbs L. Recommendations for peer-to-peer support for NICU parents. J Perinatol. 2015 Dec;35(Suppl 1):S9–13.
Fratantoni K, Soghier L, Kritikos K, Jacangelo J, Herrera N, Tuchman L, et al. Giving parents support: a randomized trial of peer support for parents after NICU discharge. J Perinatol. 2022;42(6):730–7.
Rollins NC, Bhandari N, Hajeebhoy N, Horton S, Lutter CK, Martines JC, et al. Why invest, and what it will take to improve breastfeeding practices? Lancet Lond Engl. 2016 Jan 30;387(10017):491–504.
Husebye ES, Kleven IA, Kroken LK, Torsvik IK, Haaland OA, Markestad T. Targeted Program for Provision of Mother’s Own Milk to Very Low Birth Weight Infants. PEDIATRICS. 2014 Aug 1;134(2):e489–95.
Please enter your job description and origin country
You are currently viewing a placeholder content from Facebook. To access the actual content, click the button below. Please note that doing so will share data with third-party providers.
You are currently viewing a placeholder content from Instagram. To access the actual content, click the button below. Please note that doing so will share data with third-party providers.
You are currently viewing a placeholder content from X. To access the actual content, click the button below. Please note that doing so will share data with third-party providers.